Articles / Records, patients, and staff
Do Dental Practices Need a HIPAA Risk Assessment? (2026)
A solo doctor once reported a data breach to the federal government, and ended up paying $100,000 to settle, for one document he didn't have. Here is the document nearly every dental practice is required to keep, why a checklist won't pass for it, and how to tell if you are exposed. That one document is also the groundwork the rest of HIPAA builds on, so what HIPAA actually requires of a dental practice is the place to see the whole structure.
This article explains whether a dental practice needs a HIPAA risk assessment. It is general information, not legal advice for your specific situation. For that, consult a healthcare attorney or a qualified HIPAA compliance professional.
And "your practice" includes the solo office with one dentist and a front-desk coordinator. The risk analysis isn't a suggestion or an industry best practice; it is written into the rule as a requirement, and it is typically the first thing federal investigators ask to see.
In a hurry? The free HIPAA Risk Scorecard shows you where your own practice stands in about three minutes. It is a starting point, not a full audit: Check my practice →. If you'd rather understand the why first, read on.
Here is how that plays out, and what to actually do about it.
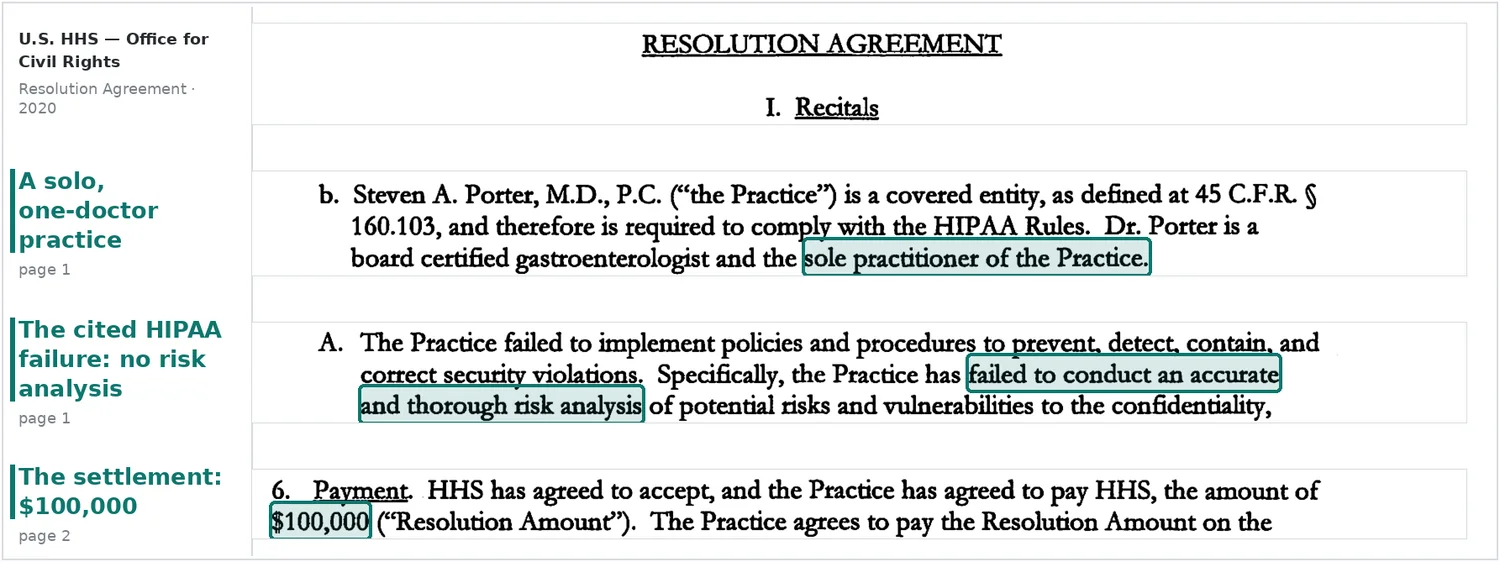
Start with that solo doctor. He was a gastroenterologist in Ogden, Utah, seeing more than 3,000 patients a year. Back in 2013 he filed a breach report with OCR: a vendor behind his electronic records system was blocking his access to his patients' data until he paid it $50,000. OCR opened a review of that complaint, and the review turned back on him: it found he had never conducted a risk analysis, and that he still had not completed one even after the agency walked him through what was required. The $100,000 settlement and two years of federal monitoring followed. (HHS Resolution Agreement, Steven A. Porter, M.D., 2020.)
He is not a dentist. But to OCR, a solo physician and a solo dentist look identical: a small covered entity holding electronic patient data, answerable to the same baseline. The lesson here isn't "don't report breaches." It's that the one document that would have protected him was the one he never had.
Is your dental practice even covered by HIPAA?
Almost certainly, and the exceptions are narrower than most owners assume.
A dental practice is a HIPAA "covered entity" if it transmits health information electronically in connection with a covered transaction: submitting insurance claims, checking eligibility, sending referrals. That captures essentially every modern office that bills insurance or uses practice-management software. The American Dental Association frames it the same way in its HIPAA 20 Questions guidance for member dentists.
A few specifics worth nailing down:
- "I'm cash-pay, so I'm exempt." Rare in practice. The moment any claim, eligibility check, or referral goes out electronically, the exemption is gone. You can also be bound contractually through a participating-provider agreement with an insurer, even without filing a claim yourself.
- "I'm solo, so this is for bigger groups." A single-location office is held to the same Security Rule standard as a hospital network. A solo dentist is also required to name a HIPAA Privacy Officer and Security Officer, and the only candidate is usually you. Not designating one is itself a documentable violation, with or without a breach.
Your practice's facts can change the answer, so for your specific situation, consult a healthcare attorney or qualified compliance professional.
So the threshold question is settled. The real question is what the rule actually demands once you're in.
What the rule says, and what OCR actually checks
The HIPAA Security Rule is organized around safeguards, and the very first administrative safeguard is the risk analysis. The text at 45 CFR § 164.308(a)(1)(ii)(A) reads:
Risk analysis (Required). Conduct an accurate and thorough assessment of the potential risks and vulnerabilities to the confidentiality, integrity, and availability of electronic protected health information held by the covered entity or business associate.
Two words in there carry the weight. "Required" means it is not in the flexible "addressable" category that lets you document an alternative. And "accurate and thorough" is the standard OCR measures you against, which is exactly where the Porter practice fell short.
This isn't a dormant rule. OCR has run a standing enforcement initiative around the right of access and around risk analysis, and its investigators consistently report that the absence of a completed risk analysis is one of the most frequent Security Rule findings when they open a file. The Porter settlement is one named example of many. So is the broader pattern: when something goes wrong, the first request is usually "show me your risk analysis," and a missing or thin one converts an incident into a finding.
There is a second, quieter point in the Porter story. He eventually got help, and still didn't produce an adequate analysis. Doing the work badly is treated much like not doing it at all. Which leads to what "the work" actually is.
The hard part isn't running the analysis. It's knowing which gaps you have before OCR does. The free HIPAA Risk Scorecard checks ten core Security Rule controls that line up with the issues OCR raises most, risk analysis and BAAs included, then you get a short written review and an introduction to a specialist if a referral makes sense. It is a starting point, not the formal risk analysis itself. Three minutes. Check my practice →
What a real dental risk analysis actually covers
A risk analysis is a documented process, not a form you sign. Done properly, it moves through a clear sequence:
Map where electronic patient data actually lives: digital X-rays and CBCT scans, intraoral photos, the practice-management system (Dentrix, Eaglesoft, Open Dental), imaging software (Dexis, iTero), billing and insurance data, cloud backups, and anything synced to a laptop or phone.
For each of those, from ransomware and phishing down to an unencrypted backup drive in a desk drawer.
Score each risk so you can tell a minor issue from a serious one.
Record the protections you have in place and the decisions you made.
Lay out how and when you will close each gap you found.
HIPAA requires the documentation to be retained for six years.
One data flow that is easy to leave out of that inventory is your own website. A booking page or contact form can send patient details to third parties through analytics or advertising code, so it belongs in the same analysis, as the rules on website tracking pixels spell out.
This is also why a generic checklist fails the test. A checklist tracks whether you have a policy; a risk analysis evaluates whether that policy actually protects the data in your environment. OCR's own guidance frames the analysis as a process specific to your environment, not a one-size-fits-all blueprint, and the practices that get cited often have a binder of policies and no real analysis behind them.
Your three options for getting it done
There are three honest ways to satisfy the requirement. None is wrong; they trade cost against confidence.
Option 1: Do it yourself with the free HHS tool.
- What it is. The federal government, through HHS and the ONC, publishes a free Security Risk Assessment (SRA) Tool that walks you through the questions.
- Who it fits. A very small, very hands-on practice with time and patience.
- The shortfall. It hands you a structure and a questionnaire. It does not tell you where you are actually exposed, it doesn't scan anything, and it doesn't track whether you fixed what you found. The output is only as good as the answers you put in, and most owners don't know what they don't know.
- Verdict. A legitimate starting point and far better than nothing. Treat it as the first draft, not the finished risk analysis.
Option 2: Lean on your IT provider or managed-services vendor.
- What it is. Your existing IT company runs or assists with the assessment.
- Who it fits. Practices that already have a capable IT partner and a signed Business Associate Agreement with them.
- The shortfall. IT skill and HIPAA-compliance skill are not the same thing. A vendor can secure your network and still miss the administrative and documentation pieces OCR weighs most heavily. And the practice, not the vendor, stays legally responsible for the result.
- Verdict. Good for the technical layer. Confirm they produce documented output you could show a regulator, not just a clean firewall.
Option 3: Bring in a HIPAA compliance specialist.
- What it is. A consultancy or compliance firm conducts the analysis and helps you remediate.
- Who it fits. Owners who want it done right once and defensible if OCR ever calls.
- The shortfall. It costs more than the other two, and quality varies, so the specialist still has to fit a solo-practice budget and workflow. (For the actual numbers, here is what a dental HIPAA risk assessment typically costs.)
- Verdict. The strongest path for defensibility. A specialist assesses your specific environment and recommends a remediation plan; they don't wave a wand and make you "compliant" on their own.
If you're not sure which path fits, that's the normal place to start. The Scorecard surfaces your likely gaps first, as a starting point rather than a full audit, so you can tell whether you can reasonably self-serve or whether you need a specialist. Check my practice →
How often, and the paperwork that proves it
The Security Rule treats the risk analysis as ongoing, not one-and-done. The practical standard most compliance professionals and federal programs use: complete a full analysis, then review and update it at least annually and whenever something material changes. A new practice-management system, a move to a new building, a staffing change with new access, or a security incident all reset the clock.
Documentation is not a side task; it is the deliverable. If OCR asks, "we did one" is not an answer. "Here is the dated analysis, the gaps we identified, the remediation we completed, and the annual reviews since" is. Keep it for six years.
What's changing in 2026, and what to do now
You have probably seen headlines about a "2026 HIPAA Security Rule." Here is the accurate status, because a lot of vendor content overstates it.
HHS published a Notice of Proposed Rulemaking in the Federal Register on January 6, 2025, proposing the first major overhaul of the Security Rule in over two decades. The comment period closed in March 2025. As of this writing, OCR has not published a final rule, and the May 2026 finalization target on its regulatory agenda has now passed without one. OCR is still reviewing the more than 4,700 comments it received, and a coalition of over 100 healthcare organizations has asked HHS to withdraw the proposal. The rule could still be finalized, narrowed, delayed, or withdrawn, so the changes below are proposed, not yet law.
If finalized, the overhaul would, among other things, remove much of the "addressable" flexibility and make safeguards like encryption and multi-factor authentication explicitly required, add scheduled vulnerability scanning, and set tighter incident timelines, like restoring critical systems within 72 hours. The direction is clearly toward less discretion and more provable, documented controls.
The practical takeaway for a solo practice is simple. The existing rule already requires your risk analysis today, and the proposed changes only raise the bar. So there is no version of the next two years where doing the analysis now is wasted effort. Build it to today's requirement, and lean toward the stricter controls the proposed rule signals.
Recommendation
Treat the risk analysis as the foundation of your HIPAA program, not a box to check before an audit. It is required now and it is among the first things OCR looks for; a missing or thin one is what turns a bad day into a six-figure settlement. For what that bad day actually looks like, see what happens when a dental practice fails a HIPAA audit and, if a breach is the trigger, what to do in the first 60 days after a breach.
Start by finding out where you actually stand. Most independent practices carry gaps they can't see from the inside. The free HIPAA Risk Scorecard checks ten core Security Rule controls that line up with the issues OCR raises most, including your risk analysis and vendor agreements, then sends you a short written review and an introduction to a specialist if a referral makes sense. It does not replace a full risk analysis, but it shows whether the broader HIPAA foundation is in place. It takes about three minutes. Check my practice →
This is general information, not legal advice. Hipsana is not a law firm, a compliance officer, or a healthcare provider. Verify current requirements with HHS or qualified counsel before acting.
About the author
Dolev Arama is Hipsana's founder. He's the one behind the Scorecard and the short risk reviews it produces. He is not an attorney, and Hipsana is a publisher and referral service, not a law firm or a healthcare provider. The writing here starts where the rules actually live (HHS, OCR, NIST) and gets checked against their current text before it goes up. Regulatory claims trace back to those sources, and figures name where they come from; anything that can't be verified is labeled rather than asserted. More about Hipsana →
Sources
- HHS Office for Civil Rights, Resolution Agreement and press release, Steven A. Porter, M.D. (2020).
- HHS Office for Civil Rights, Resolution Agreement, Elite Dental Associates (2019).
- 45 CFR § 164.308 (eCFR, current).
- 45 CFR §§ 160.103, 164.306, 164.316, and 164.530 (eCFR, current).
- HHS, Guidance on Risk Analysis (referencing NIST SP 800-66).
- Federal Register, HHS civil monetary penalty inflation adjustment, effective January 28, 2026.
- Federal Register, HIPAA Security Rule NPRM, January 6, 2025.
- American Dental Association, HIPAA 20 Questions.
Frequently asked questions
Are dental X-rays really considered protected health information?
Yes. Any information that can be tied to a patient is PHI, and that includes digital radiographs, panoramic and CBCT images, and intraoral photos. They have to be inventoried in your risk analysis and protected like any other ePHI.
What's the penalty if a dental practice gets it wrong?
HIPAA civil penalties run in four tiers based on culpability. As of the amounts effective January 28, 2026, they range from $145 per violation at the low end up to $2,190,294 per violation for willful neglect left uncorrected, with an annual cap of $2,190,294 per identical requirement. In practice, small-practice settlements are usually far below the maximum, because OCR weighs practice size along with intent and cooperation. The Porter practice settled at $100,000; a Dallas dental practice settled at $10,000. The number that should worry you isn't the statutory ceiling; it's that one of the most common triggers is so basic: no risk analysis.
Does OCR actually fine small dental practices, or just hospitals?
It does, and not only hospitals. In 2019, Elite Dental Associates, a privately owned practice in Dallas, paid $10,000 to OCR and accepted a two-year corrective action plan after disclosing patients' protected health information in replies to Yelp reviews. That was a Privacy Rule case rather than a risk-analysis case, but the point stands: OCR enforces against small dental offices.
Do I need a Business Associate Agreement with my dental lab or IT company?
If the vendor receives patient-identifiable information, yes. Labs that get patient names with cases, IT companies that can access your systems, cloud backup providers, and billing companies are business associates and need a signed BAA. A lab receiving only de-identified cases with a number may not, though that's uncommon in practice.
Can I just do the risk analysis myself?
You can, using the free HHS SRA Tool, and a careful owner can produce a reasonable first draft. The catch is that a self-assessment only catches what you already know to look for, and the gaps that sink small practices are usually the ones they didn't know they had. That blind spot is exactly what an OCR investigator finds first. Seeing where you actually stand before you decide is what the Scorecard is for.
I'm a one-dentist office. Does this really apply to me?
Yes. Size doesn't change the requirement. A solo practice must conduct the risk analysis and designate Privacy and Security Officers (usually the owner), then keep the documentation. The Porter case was a solo practice, and Elite Dental was a small one.
Not sure where your practice stands?
The free HIPAA Scorecard checks ten core Security Rule controls and scores your practice out of 100. About three minutes, no cost. A starting point, not a full audit.
Check my practice →